Finally an answer to HOW MUCH aerobic and strength training is required to lower your risk of death:

I’m at an awkward stage of life. I’m firmly in the ‘over 40’ age demographic. I love being active, doing darn near anything. Yet I have significant impediments to structured physical activity named Luke, Maeve and Nolan; my 3 kids aged 8, 6, and 4 who are in full swing of extra-curricular activities.
After 12 years of marriage I finally succumbed to my wife’s repeated requests to join a family calendar (literally yesterday) as our schedule is just getting to be too busy and I’m worried about forgetting a kid somewhere.
As you can imagine the most important commodity in my life right now is time. I need more of it and there’s just never enough.
Because of this I sympathize with every North American adult that collectively roll their eyes when they read the WHO or the US Department of Health Services recommendation of required exercise just to maintain optimal health which includes the following:
- 5-3 hours per week of moderate intensity aerobic physical activity (MPA)
- 25-2.5 hours per week of vigorous intensity aerobic physical activity (VPA) or an equivalent combination of these two
- 2 times per week of muscle strengthening exercises (MSE).
I would absolutely LOVE to exercise the minimum 7-10 hours weekly as recommended just to maintain my health, but I already wake up at 5AM six days weekly!
At this point my weekly goal is to exercise 4 times weekly for one hour each exposure. I usually average 1-2 times weekly for some semblance of cardiovascular exercise and 2-3 times per week doing strength training. Some weeks I get 3 sessions total in, others I get 5. I am way past feeling guilty about what I am accomplishing compared to the WHO recommendations because it is just works for me at my stage of life right now.
Being curious, I’ve always wondered just where the recommendations came from and if they are factually associated with a reduction in mortality. I think it’s safe to assume that everybody understands that exercise has innumerable benefits on one’s entire health profile that can be summed up with this equation I just made up:
More exercise = better health
(Trademark pending).
BUT, what I have never seen studied is exactly HOW MUCH exercise lowers my risk of dying.
I know this is a more binary definition of the benefits of exercise, but to me it’s always been a massive void in my knowledge base. Essentially I’ve always wondered the following:
“I understand that the more exercise I do the better off I am. BUT, what is the minimal effective dose of exercise I need to perform to dramatically lower my risk of dying.”
So you can imagine my absolute glee when an article that is the first of its kind confidently answered this question for me. Not only did it answer HOW MUCH exercise I need to do, but it answered how much light cardio, hard cardio, and how much strength I need to do. It even looked at combining those three forms of exercise! It also answered how much benefit I get with incremental additions of cardio and strength exercising beyond this minimal effective dose.
Let’s dive in.
This was an absolutely enormous prospective cohort study of over 416,000 American adults that completed a giant survey that began in 1957 called the National Health Interview Survey (NHIS). This massive data set is adjusted to produce a representative sample of all US civilians.
In 1997 this survey started collecting data on aerobic exercise, namely Moderate Physical Activity (MPA), and Vigorous Physical Activity (VPA) as well as Muscle Strengthening Exercises (MSE). This allowed researchers to look back at data from this point, and then compare it with the National Death Index data all the way to 2015 to see how many of these folks ended up passing away. This means it was a prospective cohort as they were able to follow these folks longitudinally to see an outcome, in this case death.
In total, of the 416,420 participants, there were 45,344 deaths.
Before I get into the results, check out these 2 items that were in the demographic data in the research paper that nerds like me notice:
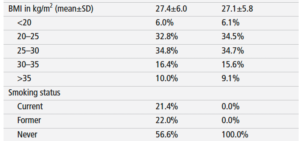
I was somewhat shocked by this! The most common BMI category is Overweight for American adults, and over one quarter of the population is either obese or morbidly obese. Also 21% were listed as ‘current smokers’? I get that this was from 1997 to 2015 but I feel like I barely know anyone that smokes anymore. Maybe that’s a positive trend?
Back to the article.
HUGE FINDING #1:
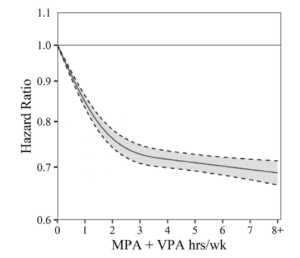
There is an inverse relationship between moderate or vigorous aerobic exercise and mortality risk at just ONE HOUR PER WEEK. The lowered mortality risk largely plateaus at 3 hours per week.
To sum this up, look at the chart below. It is showing that there is a HUGE REDUCTION in your risk of death (hazard ratio) if you complete just one hour of cardiovascular activity and it doesn’t matter if it is moderate physical activity (MPA) or vigorous (VPA). There is significant added benefit until about 3 hours weekly, and then the benefit plateaus and additional cardio show only slight benefit.
HUGE FINDING #2:
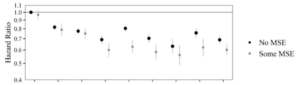
There is a significant inverse relationship between strength training and mortality risk at just ONE TIME PER WEEK but LITTLE ADDED BENEFIT beyond this frequency if the person is also doing cardiovascular activity.
Now the below chart is a bit more confusing. The x axis on the graph indicates increments of one hour for aerobic activity. The black dots show people that ONLY do cardio. The light grey ones show people that do cardio but ALSO do at least one session of strength training weekly. You can see that the grey dots are incrementally lower than the black dots at each plot along the graph, indicating that including at least one strength session further lowers your risk of death (hazard ratio). They did find that more strength didn’t really impact the graph, meaning just a single strength session is needed on top of the cardio to get the added benefit!
MODERATELY HUGE (BUT EXPECTED) FINDING:
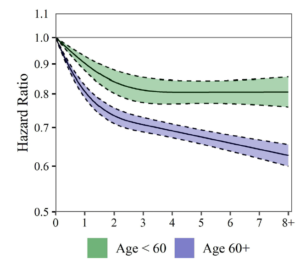
The association between aerobic physical activity and mortality risk is stronger in older folks.
When they stratified the data out by age you can see below that there is continued benefit for individuals over the age of 60 for more and more aerobic activity. For those under 60, the benefit completely levels off at 3 hours and any additional cardio did not lower your risk of death.
So what have we learned?
Before delving into our conclusions, if you feel guilty about not hitting the WHO recommendations, surveillance data in the states shows that 70% of all US adults FAIL TO MEET this recommendation. I was not surprised by this. But, one stat that I was surprised by was that 58% OF ALL AMERCIAN ADULTS currently do zero muscular strength exercise at all!
This number is alarming. We know the numerous benefits of strength training on your health (increasing bone mineral density and insulin sensitivity etc), but likely the most important benefit of strength training is offsetting age related sarcopenia/muscle loss. This causes frailty and decreased functional independence which are both major risk factors for death.
This paper was one of the first to look at strength training and mortality and is definitely the first to establish a minimum effective dose to reduce your risk of death. To sum up our strength training conclusion:
There is a marked inverse association between muscular strength training and mortality risk with as little as once weekly. There is additional mortality risk reduction when it is combined with any sort of aerobic exercise. There doesn’t seem to be much added benefit for death reduction past 1-2 times weekly (though there is definitely added health benefits). Strength training 3 times per week as we age can reverse muscle loss and improve physical functioning making us live longer.
There was a higher association with aerobic/cardio exercise where lower mortality risk is optimized at about 3 hours per week and this held true independent of your age or sex. When you dig into the data one cool observation was that it didn’t really matter what type of cardio you do whether moderate or vigorous. Both have a similar positive effect. What this means for you is that you should really just identify whatever cardio activity you enjoy and stick with that!
To sum up our aerobic training conclusion:
There is a marked reduction in mortality with as little as one hour of aerobic activity all the way to 3 hours, and then it plateaus with little added benefit for those under 65. This means the WHO guidelines are supported BUT even if you perform cardio below their guidelines you will materially lower your risk of death. It doesn’t matter what type of cardio you perform. Interestingly, the total number of bouts does not seem to matter….it’s the ACCUMULATION that matters. Even repeated 10 minute bouts confer significant benefit. It’s the TOTAL AMOUNT of time that seems to matter.
Regarding the added benefit for more and more cardio with age, the researchers think it is likely because physical activity gives people a more robust immune response and helps in the chronic conditions that occur as we age. Makes sense to me.
So don’t feel bad if you can’t hit the WHO recommendations for minimum exercise. Now we know that less exercise still offers significant benefit as it relates to mortality. Below is the final conclusion of the paper that nicely sums up all of the above:
“Regardless of sex or age, our observations suggested that: (1) Significant mortality risk reduction may result from aerobic physical activity performed 1 hour/week, with minimal additional benefits beyond 3 hours/week and (2) muscular strength training performed in combination with aerobic physical activity may further decrease mortality risk, with strength exercise performed exclusively 1-2 times/week resulting in significant mortality risk reductions.”
Now if you’ll excuse me….I have to go pick up my kids.