Lumbar Disc herniations and sciatica: strengthen your back to avoid surgery
Disc herniations in the low back are a feared outcome for many patients. That diagnosis has a bit of a reputation doesn’t it? Destined for a life of back issues, pain and eventually arthritis akin to the reputation of what an ACL tear does to the knee or a dislocation does to the shoulder. And while we wouldn’t wish a disc herniation on anyone, it does not need to be a sentence of lifelong disability that many patients unfortunately and unknowingly enable it to become.
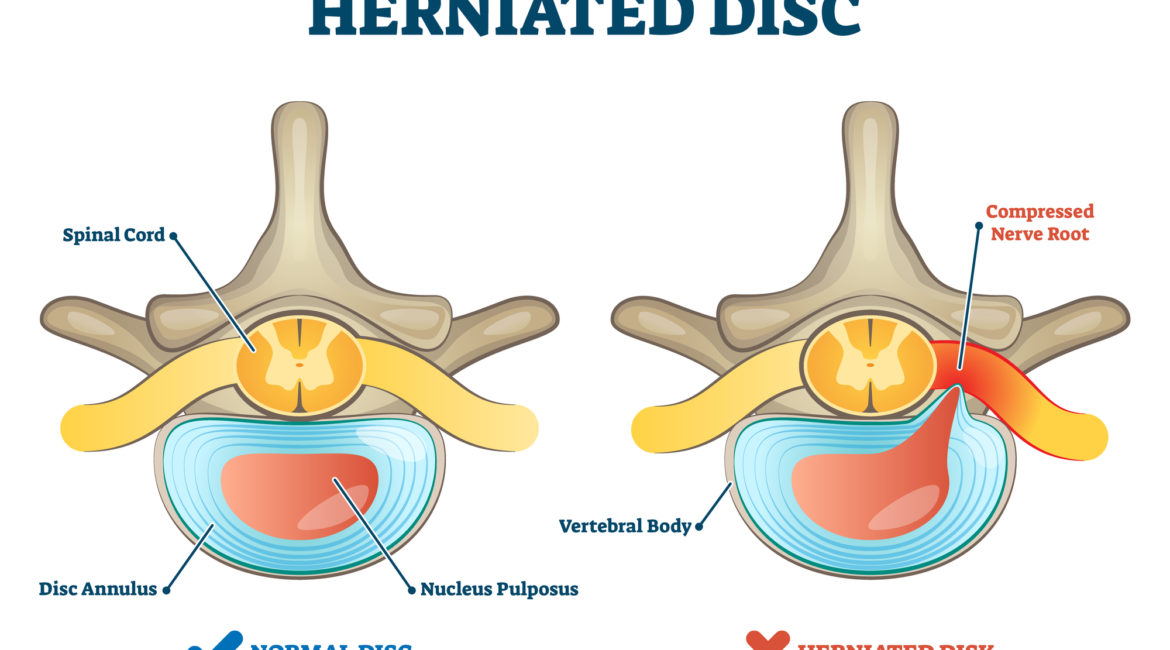
Like many other diagnoses, not all low back disc herniations are alike. There are variations in segment location (L4/5 and L5/S1 being the most common in the low back), herniation location (central, posterior, lateral) and severity. Some also affect nerves and cause pain in the buttocks, legs and feet for example (often termed sciatica). Some cause sensory disruption, loss of strength in the legs and sometimes even bowel and bladder control issues (the latter of which requires urgent attention, head to the ER!). So disc herniation patients are a broad and diverse group, which makes research and evaluation of treatment methods a challenge.
What we do know is what we see on imaging (MRI) often reverses. Spontaneous regression and reabsorption of disc herniations has been established as around 67% by Zhong et al and often occurring in the first year. (Zhong, M.; Liu, J.T.; Jiang, H.; Mo, W.; Yu, P.F.; Li, X.C.; Xue, R.R. Incidence of Spontaneous Resorption of Lumbar Disc Herniation: A Meta-Analysis. Pain Physician 2017, 20, E45–E52.) That’s encouraging isn’t it? If your orthopedic surgeon told you that, would you still go through with surgery? We’re over simplifying here of course. If you’ve followed us for any reasonable length of time you know that the structural appearance of any imaging finding is only relevant when correlated with your clinical symptoms. And in many cases there is no correlation at all. So although resorption is certainly not our clinical goal it does shine light on your body’s natural healing capacity.
You can work through it on your own, without surgery. You have options. One of those options is strength training targeted to address the deconditioning and atrophy that accompanies all low back pain cases when pain causes prolonged inactivity. Disc herniations do not differ from other causes of low back pain with regard to the local deconditioning effect on the lumbar paraspinal muscles. But in many clinical circles, disc herniation patients ARE treated differently, often inadequately addressing these physiological changes to the lumbar paraspinal muscles. Some recent research from Germany might move the needle towards a more aggressive (in terms of exercise intensity) approach.
A large clinical case series of 189 lumbar disc herniation patients has concluded that Strength training, specifically isometric back extension done in a limited range of motion, may in fact be exactly what you should be doing as a first line approach.
Published in the Journal of Clinical Medicine in May of 2021 data from a german spine centre collected from over a decade of data concluded that 9 weeks of isometric lumbar extension exercise 2 times per week can significantly improve pain and the mental health impact of disc herniations with or without nerve symptoms (sciatica/radiculopathy).
Participants in this study used a seated lumbar extension machine as seen in the image below. The angle of extension effort was determined by patient comfort. Participants built up the effort to generate a relatively high intensity isometric hold for 2 seconds, with some flexion and relaxation of the low back between each hold. The intensity of the effort was progressively increased over the course of the 9 weeks. One set of 12-15 repetitions was carried out per session. Just a couple minutes of hard work 2x/week.

In addition each patient received supervised and customized guidance of 4 other common lumbar stability and strengthening exercises (such as crunches, horizontal rows, cable pulls, reverse butterflies and lat pull downs) during their 18 sessions.
It is important to note that patients selected for this study had MRI confirmation of either a single or multilevel lumbar herniation only. Patients disqualified from inclusion in the study were patients with other visible MRI identified pathology, such as degenerative changes, stenosis, spondylolisthesis, patients over the age of 50, patients with severe loss of strength in their legs or loss of bowel or bladder control and patients whose herniation was clinically more than 3 months.
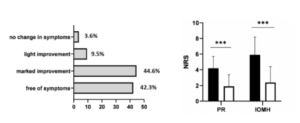
After 9 weeks 86.9% of the patients who completed the exercise protocol were completely free of symptoms or had very minor symptoms. Pretty darn good odds of success! On average pain scores (PR) were cut by more than half and impact of mental health (IOMH) scores benefited to an even greater degree after the 9 week protocol.
While this study doesn’t conclude that this type of strength training approach is necessarily better than another form of treatment or better than surgery (because it didn’t have a treatment comparison or control), it does tell us that it may be a good option for very strong short term results. And we know that 2-5 years after a disc herniation, outcomes between patients who get surgery versus those managed conservatively do not demonstrate significant differences. So you have the power, in your own body, to feel better in a relatively short period of time and preserve the anatomy you were born with.
Check out our Therapy Thursday (include link) for some guidance on how to get started on strengthening your back muscles using this isometric lumbar extension exercise approach at home with no special equipment.