Exercise therapy ‘wears down’ my knee joint: myth or reality?

“My last therapist told me to stop leg exercises because I have knee arthritis and exercising will wear down my knee joint.”
The number of times we have collectively heard this in clinic is alarming.
And it’s not the patient’s fault……the blame lies directly on the therapist.
For us, when a previous therapist tells someone the ‘wear and tear’ in their knee won’t allow them to do the things they like such as running, or strength training, we know we are fighting an uphill battle.
The idea is firmly planted in the persons head like a weed. And when they exercise it hurts! So the past therapist must be right……right?
Nnnnnnope!
A brand new article is about to come out (we got our hands on it prior to publication) that is a call to action that for once is directed to therapists and not patients.
There is a common concern amongst patients, that is amplified by out of date therapists, that for people with knee arthritis exercise therapy will ‘wear down’ their joint and repetitive or high impact activities will overload their knees and accelerate cartilage damage.
The problem?
Exercise therapy DOES NOT harm cartilage and in fact appears to IMPROVE its quality.
In fact I am going to go as far as saying MOST therapists completely ignore arthritis guidelines.
This article does a good job of summarizing the guidelines by stating that;
“…..exercise therapy plays a crucial role in managing osteoarthritis by alleviating pain, enhancing physical function, and improving overall quality of life. When prescribing pharmacological treatments for osteoarthritis, it is primarily to facilitate engagement in exercise therapy, and it is imperative to prioritize the shortest duration of pharmacological use because of limited effect and substantial side effects.”
Convinced yet?
Typically it takes about 5-10 years for research evidence to get disseminated down to clinicians.
How long have we been telling patients their knee cartilage gets adversely affected by exercise?
(Pause for emphasis)…….
54 years.
Yes. Clinicians have been telling people bullcrap for 54 years.
Speaking of bovine….the very first study looking at cartilage changes via exercise was in 1971 where a paper showed that rapid bovine loads to joins can cause rapid cartilage changes. The problem? This was on cows and with higher loads then we would ever do with exercise therapy.
Then a study on live guinea pigs and rabbits showed repeated impacts (continuous high doses of exercise that was not even natural to the animal) also degenerated cartilage.
Somehow these misconceptions led to therapists telling patients that exercise is bad for a cool half century.
But now we know exercise can actually IMPROVE cartilage.
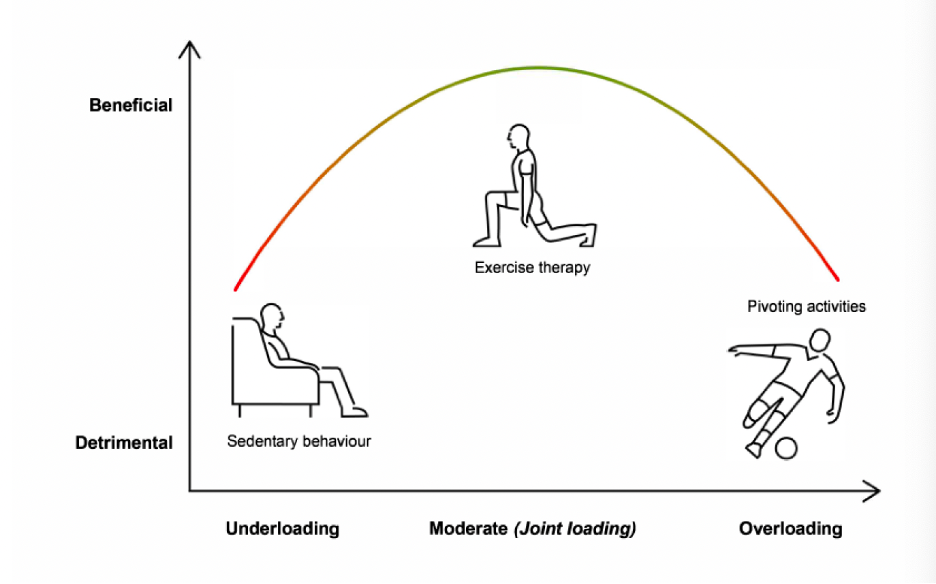
The paper does a great job of showing something we at The Proactive Athlete like to call the ‘Goldilocks approach’. This means that too little loading (sedentary behaviour) and too much loading (like high impact pivoting activities) may be detrimental to an arthritic joint. But in between is exercise therapy. In the words of Goldilocks this is ‘not too little and not too much….but just right’.
The paper cites recent review articles and papers that all show NO DETRIMENTAL EFFECTS of exercise therapy on cartilage thickness and volume, increased defects, or cartilage quality. In fact, it shows possible IMPROVEMENT in cartilage via exercise.
So what suggestions does the paper have for clinicians like us?
- We need to change our language. Instead of saying cartilage is ‘worn down machinery’ we should say it is ‘biological tissue that NEEDS regular loading to regenerate’.
- We need to assess patients beliefs about how exercise therapy may affect their knee joint cartilage by asking for instance if they are ‘concerned that exercise therapy may harm your knee joint cartilage?’
- We need to address these misconceptions about exercise therapy and let them know that TEMPORARY DISCOMFORT is ok and does not equate to long term damage to the knee joint (the most recent guidelines suggest working to a 5/10 in pain is permissible with knee degeneration!)
One final note is brought up. The paper states that while some lag is acceptable in implementing research findings, another 50 years MUST NOT pass prior to implementing this knowledge on exercise therapy into clinical practice. THIS IS THE FIRST LINE TREATMENT FOR PATIENTS WITH KNEE OSTEOARTHRITIS.
To finish, I will leave you with a wonderful analogy comparing cartilage to a sponge that does a wonderful job of educating patients about how cartilage actually works and why exercise is key to improving knee cartilage health.
“Have you ever played with a sponge? Sponges are fascinating objects that can soak up water and then release it when squeezed. They come in different shapes and sizes, and they’re soft and flexible. Inside our knees, there’s something a lot like a sponge called cartilage, which plays a vital role in keeping our knees healthy. In addition to its sponge-like properties, cartilage in our knees lubricates the knee joint, ensuring smooth movements and acting like a slippery cushion protecting the bones. However, injuries or certain conditions can sometimes cause the cartilage in our knees to become thinner or develop tiny cracks. Although cartilage doesn’t have blood vessels or nerves, it has special cells called chondrocytes. These cells are like tiny repair workers, and they help keep cartilage strong and healthy. As an example, when walking, running or bending your knee, chondrocytes start making important cartilage components like collagen and aggrecan molecules, which help repair and improve cartilage quality. Additionally, such repetitive loading activities (ie like a sponge soaking up and releasing water) promote better circulation of synovial fluid within the joint, which delivers essential nutrients to the chondrocytes and helps remove metabolic waste products. This improved nutrient supply enhances the metabolic activity of chondrocytes, supporting their role in cartilage repair and maintenance.”