The Sitting Rising Test for Longevity

Dave and I are a bit obsessed with longevity.
Ask us about research on ways to increase your lifespan and you will immediately regret it. The same way you regret asking your golf obsessed friend about their handicap……we just can’t stop talking about it!
Want some proof?
I just took a once over of our blog looking at some recent research based articles we have published on different contributors to longevity (how to live longer) or conversely to all-cause mortality (how to avoid death). Here are JUST A FEW of our favorites from the recent past.
How VO2Max helps predict longevity
The Nicoya Costa Rica secrets to longevity
On sugary coffee and longevity:
On Metabolic Equivalent of Task (METS) to live longer
On walking speed as a predictor of longevity
On fasting (we have lots of blogs on fasting if you search our website)
On red meat intake and longevity
On cardio versus weight training to help you live longer
On why walking is even more important that quitting smoking for all cause mortality
On Grip strength as a predictor of longevity
On knee and hip OA as a predictor of death
Believe me now?
Well get ready to be subjected to the crème de la crème. We stumbled upon a single test that is generally predictive of longevity, and at the same time EXTREMELY frustrating.
Let me introduce you to the Sitting Rising Test and explain why it may help predict how likely you are to die.
Seem morbid? Well read on.
The sitting rising test was actually first described in the late 1990s but was first published about in 2012 from a Brazilian research group.
They had one specific mandate; to develop a simple, reliable and valid physical test that was able to predict a person’s longevity and functional decline.
We have known for decades of some physical traits that are linked with all-cause mortality like cardiovascular fitness and grip strength (see blogs above). What has been missing is a single test of general functionality, meaning a test of combined physical parameters like strength, power, flexibility and balance. The researchers argue that these parameters are more closely linked to outcomes that WE KNOW greatly increase your risk of death like falling, or the inability to stand up from a chair.
Let me introduce you to the sitting rising test.
The test itself is simple. The researchers even made a great short video explaining the test as well as the scoring (note the video is in Brazilian so has subtitles). We also made a short video where I put Dave through the test here.
The basis is simple. You instruct someone to try and sit down and then stand up without having to use their hands or legs for any sort of support. You are allowed to cross your legs to lower yourself to the ground and then rise back up to standing. For each support you have to use (like placing one hand on your knee or the ground) you lose one point. You also lose 0.5 point if the assessor judges that you lose your balance. Your total is out of 10 full points (5 for lowering to sitting, and 5 for rising back to standing).
Sound easy?
Try it. I dare you.
If you take a few tries, that is fine. The assessor is meant to take the best total score (added between 5 points for sitting down and 5 for standing back up).
The controversy with the sitting rising test is on the validity of the test. Can it actually predict anything?
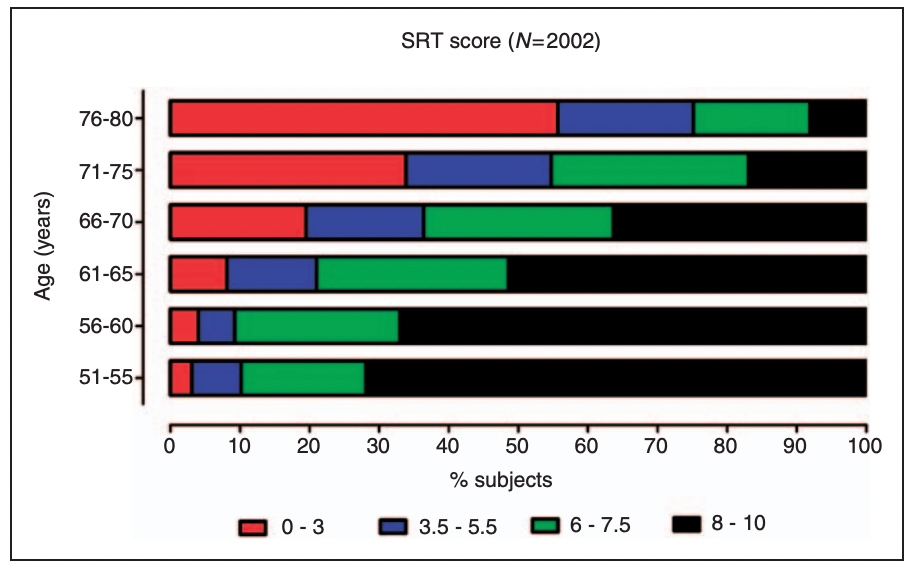
Well the first study in 2012 was a retrospective cohort study from 1997 through 2011. Essentially they took 2002 (68% male) participants all aged 51-80, had them perform the sitting rising test, and followed them for a median of 6.3 years to see how many died.
Now there are a couple of caveats with this study. First, they excluded the two ‘long tail’ parts of the population curve, meaning those in great shape by excluding anyone that regularly competed in sporting events, as well as those that presented with any relevant MSK limitations that could affect the performance of the test. This means that only the ‘middle of the population curve’ was represented by the study, which isn’t really reflective of the population at large. This immediately should question the tests utility across a broad swath of the population.
Back to the study. Overall the death rate was 7.9%. What matters is the distribution of the test. To assess this the researchers split the participants into 5 year age intervals seen below.
Here are the pertinent findings:
- Of the 2002 total people followed, just two people that scored a perfect 10 died (one male aged 64, and a female aged 54).
- NOBODY over aged 70 scored a perfect 10.
- When they statistically remove age, gender and BMI in the analysis, the researchers found there was a 3 year shorter life expectancy among those in the lowest score category versus those in the best category.
- Those in the lowest score range have a 5-6 fold higher risk versus a reference group.
- With each increment in test score improvement, there is a 21% reduction in all cause mortality!
- From this study, the researchers stated that a partial score of 4/5 (8-10 total) in the test will preserve functional independence in an individual regardless of age as they feel this will reduce your risk of falls. So essentially that is the minimum score you should strive for.
Here is another useful chart that better depicts your survival rate based on your initial score that I think is useful:

This initial study got a ton of publicity, but also raised some further questions. The researchers then re-published in 2020 in Preventative Cardiology but it was just a more robust set of reference data and wider age range. Inexplicably, again they excluded athletes. This time there were 6141 adults aged 16-98.
Nothing was terribly surprising in this study. For instance a 10/10 is the most common score for men aged 16-25 and for women aged 16-40 (way to go women!). On the other side, less than 8% of men and women aged 55 and over achieved a 10.
Because of the more robust data set the researchers were able to discern what age the test becomes discriminative meaning where the test starts to become predictive and important. For men, this was from age 46 to 80 and in women from ages 46 and 75. I believe this is because the majority of people younger than this all get a similarly high score.
So is this test actually useful?
I think so. But I also think its findings have been way overblown.
It is a wonderful, easy to administer test for ones functional capacity. And that is very important and often neglected as we age. In fact, falls are the leading cause of unintentional injury related deaths for people aged 65 and over.
To me the test is a simple measure of mobility and strength. Sarcopenia (muscle loss) is a major factor in longevity. So is balance and range of motion. The sitting rising test measures all 3.
There are many simple to administer tests for longevity and my guess is scoring high on a broad swath of them is more important than any single test on itself.
Another thought is that it can be used as an objective measure. If you score suboptimal, there is absolutely no reason 3-6 months of training would not see you materially improve your score.
Now if you’ll excuse me, I have some mobility work to get to.